


Upper Cervical Concepts

Dan Murphy, DC
Private Practice of Chiropractic;
Diplomate American Board of Chiropractic Orthopedist;
Faculty Life Chiropractic College West;
Vice President ICA 2003-2009;
ICA Chiropractor of the Year 2009
INTRODUCTION
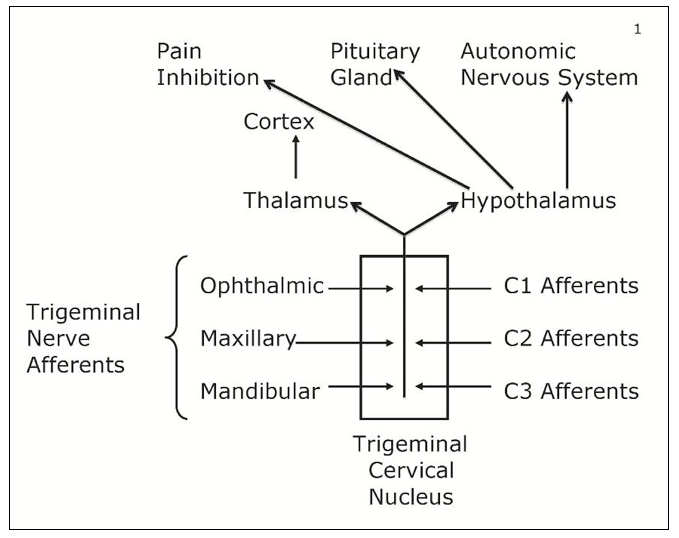
A key component to understanding the upper cervical spine is to understand the Trigeminal-Cervical Nucleus. In his 1995 article Nikolai Bogduk, MD, PhD1 makes these points:
The point is that the trigeminal nerve afferents and the upper cervical afferents are neuro-mechanically linked. Upper cervical spine afferent mechanoreceptors arising from the capsules, ligaments, and discs are well documented. Importantly, the sub-occipital muscles are documented to be the most densely innervated (by far) with muscle spindle mechanoreceptors.2
- Neuroanatomical Pathways
“Our first conscious muscular act is nursing at the breast. The neuronal pathways mediating and stipulated by nursing from the beginnings of our awareness of ‘self’ as well as the neuronal substratum upon which all future emotional and mental experience is interpreted and recorded. The tactile and oral sensations that accompany this extremely important act, namely pleasure, warmth and security, are conveyed centrally primarily by the trigeminal nerve, the trigeminal sensory nuclei in the brain stem, the trigeminal tracts, the nucleus VPM [ventral posterior medial] in the thalamus and its myriad connections.”
“Conceivably whether a person is basically happy and content in life, whether he or she is trusting of others human beings, and whether he or she is capable of loving another human being may all depend upon the sufficient stimulation, activation and persistence of these neurons, their connections and their neurotransmitters.”
- The Brain and Behavior:
There are monosynaptic inputs to the hypothalamus that arise from within the trigeminal spinal nucleus. “These fibers project directly to many areas of the hypothalamus. The monosynaptic pathways provide a route for reflex autonomic and endocrine behaviors.”
- Integration
The central nervous system (spinal cord, brain stem and brain) is built upon the quality of its afferent (sensory) stimulation. Apparently the first and most important sensory afferent input for the development of the synaptic array of the spinal cord, brain stem, and brain is to the trigeminocervical nucleus. The quality of the input into the trigeminocervical nucleus is ultimately linked to the following:
- Headache perception
- Emotional and mental experience
- Happiness and being content in life
- Trusting of other human beings
- Being capable of loving another human being
- Autonomic (visceral) nervous system function
- Endocrine hormonal function
DISCUSSION
The KEY is the understanding that the sensory afferent input into the trigeminocervical nucleus originates from two primary sources:
1) Mouth/temporomandibular function (TMJ)
2) Upper cervical spinal mechanical afferentation
These concepts are well supported by German physician Heiner Biedermann, MD.3-5
SUMMARY
The powerful systemic influences of upper cervical chiropractic improvement of mechanical afferentation is linked to the most important mechanical (not to mention nutritional) influences on central neurological development: breast feeding.
References
1) Nikolai Bogduk, MD, PhD Anatomy and Physiology of Headache Biomedicine and Pharmacotherapy; 1995, Vol. 49, No. 10, 435-445.
2) Boyd-Clark et. al., Quantitative Study of Muscle Spindles in Suboccipital Muscles of Human Foetuses; Neurology India, 2001, 49, 355-359.
3) Kinematic Imbalances Due To Suboccipital Strain In Newborns. Journal of Manual Medicine; June (No. 6) 1992, pp151-156.
4) Manual Therapy in Children, Churchill Livingstone; 2004.
5) Manual medicine of functional disorders in children. Medical Veritas: The Journal of Medical Truth; 2006; Vol. 3; pp. 803-814.
 CBP Seminars
CBP Seminars
