


Lumbar Spine Ergonomics Part 2: The 5 Key Contemporary Concepts
 Paul A. Oakley, M.Sc., DC
Paul A. Oakley, M.Sc., DC
CBP Research & Instructor
Private Practice New Market, Ontario, Canada
INTRODUCTION
Last issue we discussed the essential reasons for the understanding of contemporary ergonomics concepts and their potential contradictory effects on patient care – good ergonomic practices will aid in patient response to care - poor ergonomic practices will undeniably compromise patient outcomes. We have discussed the first two concepts, and now continue with concept 3 of 5.
3) Optimal Spinal Loading: Not too Much, Not too Little
A common ergonomic misconception is that recommendations should be directed at minimizing tissue loading, however, this is not true.1 For example, not typically considered stressful to the spine, sleeping for more than 8 hours at a time may indeed stress the spine.1 This is due to the fact that the discs swell by imbibing fluid over night,2 and since the discs function to transmit force, (rather than absorb force which is the function of the vertebral bodies)3 the column is subjected to increased stiffness and is at greater injury risk in the early morning.4 The fact is too much loading or too little loading is potentially injurious. For this reason, “the challenge is to develop a wise break strategy to facilitate optimal tissue adaptation.”1
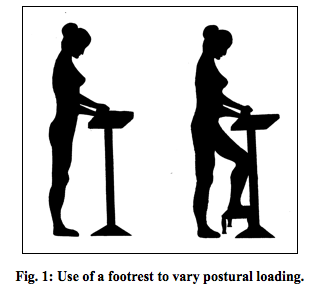
Since most spinal injury occurs as an accumulation of micro-trauma as opposed to an isolated acute traumatic event,5,6 regular ‘micro-breaks’ are recommended. This allows a continuously varying demand and subsequent migration of load on the low back tissues.1 Standing up to answer the telephone while performing seated work is a good way to aid in varying the posture throughout the day. Any posture adopted for prolonged periods may fatigue the tissues used to maintain that position. When standing for long periods one can alternate the placement of a foot on top a footrest to reduce tension in the psoas and lumbar spine.7 See Figure 1.
The idea of an ideal sitting posture is a farce. This is because it would only be ideal for about 10 minutes1 as sitting creeps the posterior ligamentous tissues (20 minutes of continuous sitting requires over 30 minutes of non-seated recovery time to regain the normal protective spine stiffness8). The ideal sitting posture is a variable one.9,10 McGill (2002)1 suggests three recommendations for prolonged sitting: 1) Use an ergonomic chair properly (i.e. vary the adjustable features regularly within sensible ranges); 2) Get out of the chair (i.e. rest breaks should involve opposite activities – Mirror Image Postures); 3) Perform an exercise routine during the workday (i.e. not first thing in the morning; not exercises that exert excessive spinal loads).
4. Reduce the Reaction Moment
The ‘reaction moment’ is the rotational force your body must generate to successfully perform a sagittal lift - the weight of the load (and upper limbs) would cause your torso to fall forward unless the back extensors offset this gravity-induced moment to allow the maintenance of an upright lift. The extensor activity within the low back causes compression of the spinal mechanism.11 Excessive compression within the low back is detrimental especially during prolonged, or repeated tasks. Excessive loading of the low back due to reaction moments can occur during any activity where there is a demand for the body to resist a force that is a distance from the spine.
Reducing the reaction moment is the key to reduce spinal compression. This is accomplished by carrying the load closer to the body and/or reducing the weight of the load lifted. See Figure 2.
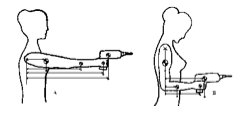
Fig. 2: Reduction of ‘reaction moment’ and therefore muscle work is accomplished by bending the arm to decrease distance of arm segments and load from spinal axis.
A third method of reducing a reaction moment is to direct the transmissible vector through the low back. The ‘transmissible vector’ is likened to the former concept only applied to tasks such as pushing and pulling. It should be known that there is no specific muscle that has the primary function of producing torso torque, it is performed by co-contraction of all the torso muscles resulting in substantial spinal loads.1 Thus, when performing tasks such as pushing and pulling on objects such as doors and vacuums, the pull/push should be directed so that it is in line with the low back.
5) Maintain Spine Stability
McGill was the first to capture a ‘live’ segmental spinal buckling while viewing the spine of a power lifter during a lift.12 This buckling is possible when either there were high forces in the global muscles and low forces in segmental muscles or when there are low forces in all muscles.13 This mechanism explains how one can injure themselves by performing ‘negligible’ lift such as picking up a pencil.5
As expressed by McGill, “stiffness creates stability,” and symmetrical stiffness offers greater stability.1 Thus, a slight abdominal co-contraction (5-10% max. vol. contraction) will ‘brace’ or stabilize the spine prior to a lift. This will prevent any tissue from bearing a surprise load.14 Spinal stability is also maintained by adopting symmetric postures, avoiding twisting action, and flexion postures. Symmetrical trunk postures also ensure greater available strength,15 enabling one to perform activities easier in symmetric postures.
Lastly, the lumbar lordosis is essential in maintaining spinal stiffness – keeping it dynamically (lifting) and having it statically (standing) – any chiropractic treatment neglecting the correction of lumbar lordosis is missing a key ingredient for their patient’s back stability and health.
Conclusion
It has been suggested that the “mechanics of the spine are not well understood by those who examine and treat these structures.”16 The Chiropractic BioPhysics® lumbar rehabilitation protocol has its unique niche in remolding the spinal posture and thus succeeding where most other LBP treatments fail including other chiropractic techniques. Both the neutral static posture and the dynamic postures performed throughout the day have significant implications for spinal health and response to treatment. The performance of a lumbar rehabilitation without regard for the dynamic activities performed throughout the day may render patient care fruitless. Always consider the Five Key Concepts to Lumbar Spine Ergonomics:
1. Maintain the Neutral Lumbar Curve
2. Appropriate Timing of Spinal Loads
3. Optimal Spinal Loading: Not too Much, Not too Little
4. Reduce the Reaction Moment
5. Maintain Spine Stability
References
1.McGill SM. Low back disorders: Evidence-based prevention and rehabilitation. Champaign, IL: Human Kinetics, 2002.
2.Urban JPG, McMullin JF. Swelling pressure of the lumbar intervertebral discs: Influence of age, spinal level, composition, and degeneration. Spine 1988;13:179-187.
3.Ruch WJ. Atlas of common subluxations of the human spine and pelvis. New York: CRC Press, 1997.
4.Adams MA, Dolan P, Hutton WC. Diurnal variations in the stresses on the lumbar spine. Spine 1987;12:130-137.
5.McGill S. The biomechanics of low back injury: implications on current practice in industry and the clinic. Journal of Biomechanics 1997;30:465-475.
6.Kumar S. Cumulative load as a risk factor for back pain. Spine 1990;15:1311-1316.
7.White III AA, Panjabi MM. Clinical biomechanics of the spine. 2 ed. New York: Lippincott Williams & Wilkins, 1990.
8.McGill SM, Brown S. Creep response of the lumbar spine to prolonged full flexion. Clinical Biomechanics 1992;7:43-46.
9.Eklund J. Biomechanical aspects of work seating. In: Kumar S, ed. Biomechanics in Ergonomics. Philadelphia: Taylor & Francis, 1999:325-334.
10. Pynt J, Higgs J, Mackey M. Seeking the optimal posture of the seated lumbar spine. Physiotherapy Theory & Practice 2001;17:5-21.
11. Troup JDG. Relation of lumbar spine disorders to heavy manual work and lifting. Lancet 1965;857-861.
12. Cholewicki J, McGill SM. Lumbar posterior ligament involvement during extremely heavy lifts estimated from flouroscopic measurements. Journal of Biomechanics 1992;25:17-28.
13. Cholewicki J, McGill SM. Mechanical stability of the in vivo lumbar spine: Implications for injury and chronic low back pain. Clinical Biomechanics 1996;11:1-15.
14. McGill SM, Norman RW. Low back biomechanics in industry: The prevention of injury through safer lifting. In: Grabiner MD, ed. Current Issues in Biomechanics. Champaign, IL: Human Kinetics Publishers, 1993:
15. Kumar S, Narayan Y, Zedka M. An electromyographic study of unresisted trunk rotation with normal velocity among healthy subjects. Spine 1996;21:1500-1512.
16. Paris SV. Anatomy as related to function and pain. Orthopedic Clinics of North America 1983;14:475-489.
 CBP Seminars
CBP Seminars