


Combining Specific Chiropractic Adjusting Techniques with CBP Corrective Care Techniques

 Todd Pickman, DC
Todd Pickman, DC
Private Practice of Chiropractic Eagle, ID
Gonstead Technique & CBP Trained Chirorpactor
 Deed E. Harrison, DC
Deed E. Harrison, DC
President CBP Seminars, Inc.
Vice President CBP Non-Profit, Inc.
Chair PCCRP Guidelines
Editor—AJCC
INTRODUCTION
We've all heard the Chiropractic adage that 'all techniques work'. This is likely true but we first need to define what is meant by the term 'works'. If we assume that what is meant by 'works' is that all techniques are able to improve joint mobility, posture mobility, and reduce pain and muscle hyper-activity by reflexo-genic inhibitor effects, then this statement holds some merit. However, certain specific segmental adjusting techniques have more research validating this statement than others. For example, using the Gonstead Technique system of analysis and adjusting, Nansel and colleagues1 found statistically significant improvements in cervical lateral bending motion responses following one specific adjustment to the restricted side of the cervical spine.
In contrast, if we assume that what is meant by 'works' is that all techniques are able to improve the alignment of generalized abnormal sagittal plane curvatures, then this statement does not hold merit. For example, using the same Gonstead Technique system of analysis and adjusting, Plaugher et al2, found no measurable change in the cervical and lumbar lordosis in 50 patients receiving several adjustments. Regarding CBP Technique corrective methods, statistically significant improvements in sagittal plane alignments have been identified in several clinical control trials examining patients suffering from chronic low back and cervical spine disorders.3-6
So what does the above information indicate? In our opinion, the above indicates that the astute Chiropractor should become skilled at administering both a segmental specific adjustment technique and a full spine corrective technique like Chiropractic BioPhysics (CBP). In this manner, patients will experience the benefits of segmental motion restriction improvement and the restoration of proper full body and spine alignment. The case presented herein attempts to provide initial rationale for the combination of two uniquely distinct, but complimentary full spine Chiropractic Technique systems.
Case Study:
Approximately, 6. 5 years ago (in 2006), a 74 year old female presented to one of the author's (T.P) practices seeking care for the relief of functional disabilities related to a chronic low back condition. At this time, the Chiropractic clinician (T.P) exclusively adhered to and utilized the Gonstead Technique system of analysis and adjusting for identified spine subluxations including:
- Abnormal temperature differential patterns (nervo-scope / tempo-scope).
- Static palpation data indicating the presence of edematous tissue around the injured segment.
- A decrease in motion of the segment in question, as compared to the surrounding area.
- Palpable muscle spasm or splinting around the area in question.
- Visualization of the area (looking for presence of pitting edema, asymmetry in the tissues, etc).
- Then, consulting the 3-shot, digitally stitched, AP full spine x-ray and the lateral (2 shot) full spine x-ray to analyze the “foundation principle” and relate this to the examination findings.
At this time, the patient was recommended and consented to a program of care consisting of Gonstead adjustments at a frequency of 3 times for 2-weeks, 2 x per week for 4 weeks, and then 1 x per week for 6 weeks. At this point the patient was improved to some extent (not completely) and was placed on a Chiropractic maintenance schedule consisting of 1-4 x per month sessions of adjustments over the course of 6 years. Through the course of this 6-year time period the patient would have episodic acute flare-ups of her chronic low back conditions that would improve with Chiropractic. The patient averaged a minimum pain intensity of 4/10 over the course of these 6-years with flare-ups reaching 8/10 on a numerical rating scale.
- Feb 2012 Findings: In February of 2012, the Chiropractor (T.P.) informed the patient that he had learned a new approach to full spine corrective Chiropractic (CBP Technique) and that he believed she was a candidate for this 'new' system. The patient was recommended and consented to a 36 visits, 3-month, corrective care program consisting of the combination of Gonstead Technique (segmental adjusting applied to the cervical, thoracic, and lumbo-pelvic regions) and CBP Technique. Her pain scale was a 7/10, she reported difficulty walking more than 1/4 mile distances without severe thoraco-lumbar pain, fatigue, and spasm, all while wearing a back brace.
- Radiographic Findings:
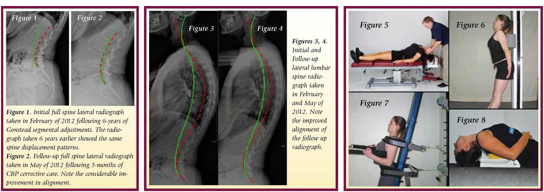
Lateral Full Spine Radiograph: In February, 2012 a new digital full spine lateral radiograph of the patient was obtained. See Figure 1. The radiographic analysis was done using the PostureRayÒ computerized radiographic measurement system. Qualitatively, the patient’s radiographic displacements are shown in Figure 1 as the path of their posterior vertebral body margins from C2-S1 relative to an idealized spine model in upright stance developed by Harrison and colleagues.7 The patients follow up full spine lateral radiograph after 3-months of CBP Technique is shown Figure 2. Note the remarkable improvement in alignment, whereas previously, for 6 years no such improvement was identified with Gonstead Technique alone.
Lateral Lumbar Spine Radiograph: In February, 2012 a digital lateral lumbar radiograph was obtained. See Figure 3. The radiographic analysis was done using the Posture RayÒ computerized radiographic mensuration system. The patient’s radiographic displacement values are shown in Figure 3 and are compared against normal.7 The patients follow up full spine lateral radiograph after 3-months of CBP Technique is Figure 4. Note the remarkable improvement in alignment where for 6 years no such improvement was identified with Gonstead Technique alone.
Interventions: The primary course of interventions included CBP mirror image® adjustments, exercises, and traction to reduce her full spine postural and spine displacements. The treatment frequency was 3 times per week for 40 visits over approximately 12 weeks. The Patient presented to and actively participated at all appointments. Each visit consisted of mirror image adjusting, mirror image exercises and traction to reduce her abnormal posture displacements.
- Mirror Image Adjustments
The patient was administered mirror image adjustments to correct posterior thoracic translation with hyper-kyphosis and anterior head translation with head flexion postures. See Figures 5.
- Mirror Image Exercises
The patient was administered mirror image adjustments to correct posterior thoracic translation with hyper-kyphosis and anterior head translation with head flexion postures. See Figures 6.
- Mirror Image® Traction
Mirror Image traction care was administered to the patient. The patient received traction in the standing posture as shown in Figure 6. In addition the patient was instructed in the use of the denneroll thoracic orthotic and was advised to do this 5-7 times per week at home. See Figure 7.
- Case Outcome Subjectively, at the end of the 1st month of corrective care, the patient was remarkably improved; NRS = 1-2 / 10. Her low back condition improved to where she was able to walk 3-miles without the use of a low back support and without debilitating pain. According to the patient, in her own words, "I do know that I'm experiencing a life change for the better...I'm singing the praise for the treatment (CBP Technique--added for clarity) and how great I feel".
CONCLUSION
The authors' opinion is that the patient's improvement is directly related to the spinal corrective procedures applied using CBP Technique. Accordingly, for optimum patient response, traditional Chiropractic adjustments would seem to be enhanced by the addition of spinal corrective procedures as in CBP. In the end, it is the positive response of the patient that should dictate this combined approach of classical Chiropractic care, with more contemporary corrective Chiropractic systems.
References
- Nansel DD, Cremata E, Carlson J, Szlazak. J Manipulative Physiological Ther 1989;12:6:419-427.
- Plaugher G, Cremata EE, Phillips RB. J Manipulative and Physiol Ther 1990.
- Harrison DD, Jackson BL, Troyanovich SJ, Robertson GA, DeGeorge D, Barker WF. J Manipulative Physiol Ther 1994;17(7):454-464.
- Harrison DE, Cailliet R, Harrison DD, Janik TJ, Holland B. Archives Phys Med Rehabil 2002; 83(4): 447-53.
- Harrison DE, Harrison DD, Betz J, Janik TJ, Holland B, Colloca C. J Manipulative Physiol Ther 2003; 26(3): 139-151.
- Harrison DE, Harrison DD, Cailliet R, Janik TJ, Holland B. Arch Phys Med Rehab 2002; 83(11): 1585-1591.
- Harrison DE, Harrson DD, Haas JW, Oakley P. Spinal Biomechancs for Clinicians, Vol I. Evanston, WY: Harrison CBP Seminars, Inc., 2003, ISBN 0-9721314-2-6.
 CBP Seminars
CBP Seminars